
https://www.curamedix.com/blog/shockwave-therapy-as-the-ultimate-healing-accelerator
Check out this simple, effective explanation of the benefits of Red Light Therapy. Then, come use mine at my practice.
Radial extracorporeal shock wave therapy-new service offered!
Extracorporeal Pulse Activation Technology (EPAT) is an advanced and highly effective non-invasive treatment method cleared by the FDA for certain musculoskeletal injuries. This technology is based on a unique set of pressure waves that stimulate the metabolism, enhance blood circulation, and accelerate the healing process of damaged superficial tissues like the achilles, plantar fascia, neuromas, elbow injuries, rotator cuff tendons and even stress reactions of the tibia. Youth injuries like Osgood Schlatter Syndrome and Sever’s Disease are difficult to treat and they take time, appropriate home exercises, and avoiding too much impact while healing. The EPAT device not only helps to alleviate pain but to repair the damaged tissue to facilitate return to play faster.
The beneficial effects of EPAT are often experienced after only 3 treatments but may require up to 6 treatments at 1x per week. Some patients report immediate pain relief after the treatment, although it can take up to 4 weeks for pain relief to become quite noticeable. As is always standard care in my Physical Therapy practice, appropriate exercises and stretches are instructed to maximize healing.
Check out the evidence!
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5674749/
https://pubmed.ncbi.nlm.nih.gov/33367924/
https://pubmed.ncbi.nlm.nih.gov/30412072/
https://pubmed.ncbi.nlm.nih.gov/30068324/
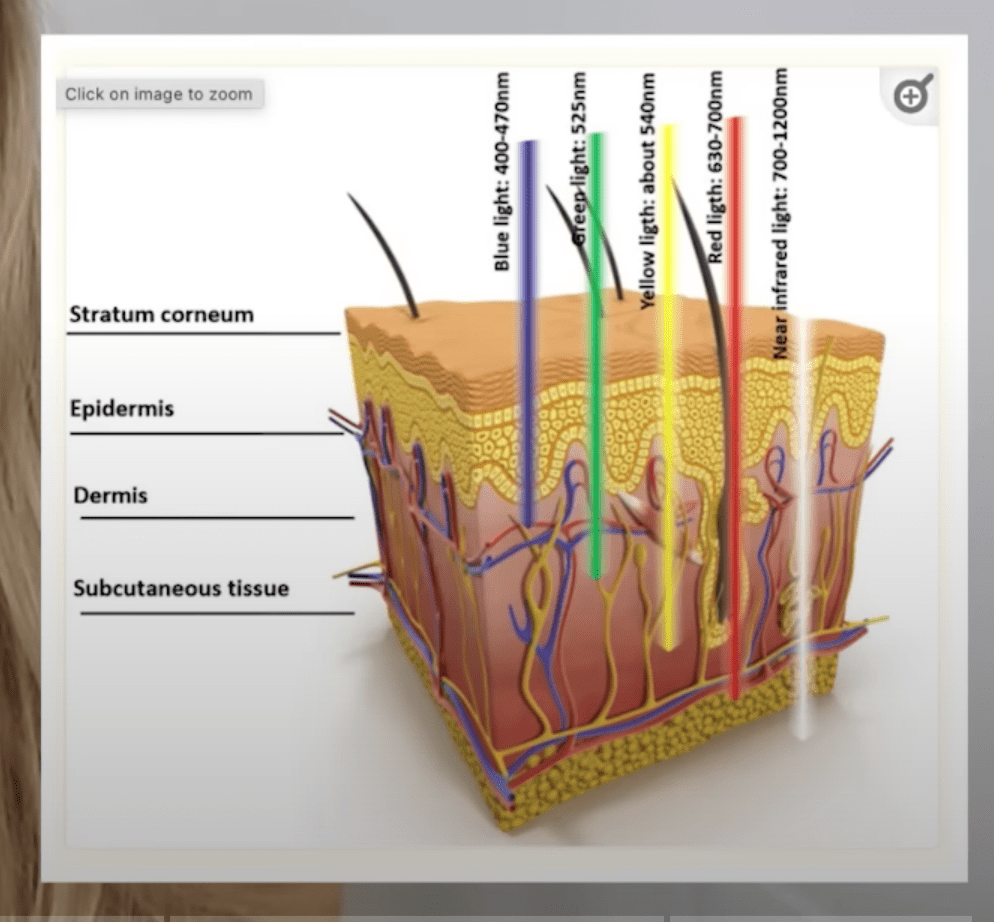
Red Light Therapy
Red Light Therapy (RLT) as a potential for healing is not a new concept but in the last decade, research has exploded whereby there are over 5,000 studies published. There is now evidence supporting the cognitive, sleep, mood, post work out recovery, weight loss and musculoskeletal pain benefits. Mitochondria, the “power house” organelle in most of the tissues in our bodies, benefits greatly from RLT. Energy produced by mitochondria is stored in a molecule called adenosine triphosphate ATP. ATP is involved in every biological process in our bodies and works to repair tissue. ATP activity is increased with RLT as it communicates with other brain signaling pathways. RLT therapy includes a whole spectrum of light energy but only Infrared (IR) and Near infrared (NIR) wavelengths of light energy penetrate past our skin into deeper tissues. When used correctly in terms of dosage, with use of a quality LED device, this is a safe and effective tool to augment other Physical Therapy interventions.
Using the RLT just means standing or sitting 10-12 inches away from the panel with protective eyewear worn. The area on your body you would most like to address is exposed to the LED lights. This device can be used 5 days per week, safely, but can still help to hasten recovery once. Every individual has different needs and I encourage you to reach out with questions at any time.
Contraindications: While my panel is a non-thermal device, people taking medications that cause photosensitivity and those who are pregnant should not use this device out of an abundance of caution.
- https://pubmed.ncbi.nlm.nih.gov/27973730/
- https://pubmed.ncbi.nlm.nih.gov/29164625/
- https://pubmed.ncbi.nlm.nih.gov/28748217/
- https://pubmed.ncbi.nlm.nih.gov/28441605/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2790317/
**If you would like a RLT panel for home use, I only recommend a brand that fully discloses their testing techniques, provides full speculations, has good customer service and a warranty. I recommend a few reputable sources and one of them is Hooga. I have a Hooga brand panel and I can guide you on what would be most appropriate for your needs. In addition, here is a 12% discount if you choose Hooga.
Space to sublet here in my office suite! Body workers, healthcare, wellness folks-please inquire.
Squat correctly to save your joints!
Craig’s Test for the hip
Concussions: post concussive rehabilitation options
Concussions differ so widely that it takes skilled health care providers and trainers to properly assess, treat and make decisions on return to play (RTP) with a variety of assessment tools. Remember that nerve cells in the brain are extremely fragile and vulnerable to re-injury at this time and there are good systems in place to minimize the individual’s risk of further damage. Premature mental tasks, physical tasks and stress delays healing and therefore direct communication amongst school staff, coaches, trainers, physical therapists and providers offers maximum success for a full recovery.
Once the person’s symptoms have subsided at rest and with mental challenges (headaches, dizziness, visual disturbances, increased sensitivity to light and sound, agitation, loss of memory, uncoordinated movements and loss of balance are examples), they are likely ready for conditioning. According to the American College of Sports Medicine and other published literature on the safety and efficacy of the rehabilitation process, the following 5 day progression can be implemented.
Day 1: Light aerobic exercise for 5-20 minutes which can include a stationary bike, stair climbing, rowing, a brisk walk, or elliptical machine, to name a few options.
Day 2: Aerobic exercise at moderate intensity and to continue up to 20 minutes, as tolerated
Day 3: Interval training, sprinting or otherwise high intensity aerobic exercise
Day 4: Contact exercises begin but in controlled, supervised setting
Day 5: Return to sports without limitations/restrictions
It is so important it bears repeating that this is not “one size fits all.” Individuals must be assessed all along to observe for any changes in coordination, balance and ability to concentrate and follow directions, as well as be symptom free.
Concussions: a few facts to keep in mind
Concussions are a common topic as regulations are in place amongst team sports in the United States. Information floods the internet for parents, coaches and caregivers, and for the lay person, this can be overwhelming. My goal here is to highlight a few facts and offer suggestions to help avoid unnecessary dangers to kids having had suffered a concussion.
Concussions can happen by any blow to the body which results in a disruption to a normally functioning brain and causes neuronal shearing. This may not include a hit to the head (less than 10%) and often does not include unconsciousness. Most incidents include a resolution of symptoms in 2-3 days. Also, whiplash associated disorders (WAD) are common in conjunction with concussions due to the rapid deceleration of the neck on the head. Symptoms from WAD can take longer to subside.
Typical complaints after concussion include, but are not limited to, headaches, nausea, dizziness, balance issues, difficulty with memory, depression, double or blurred vision, light/noise sensitivities, confusion, and sluggishness. Furthermore, what a coach, parent or friend might see are clumsy movements, mood changes, personality changes and/or difficulty answering simple questions.
Here is what everyone needs to know and follow. Any person who is suspected of suffering a concussion needs to be systematically evaluated by a trained health care provider and at that point determined if imaging of the brain and/or neck is warranted. The good news is that the examination is thorough, objective and offers a lot of information very useful for rehabilitation purposes, should that need arise. Only after this evaluation will it be determined if the person is safe to return to play (RTP). Because the nerves in the brain are injured, they are very susceptible to re-injury and the likelihood of long term damage rises. Multiple concussions are dealt with much more conservatively as the health risks rise. Almost half of athletes do not report symptoms after suffering a concussion. Be aware and on the lookout for symptoms and complaints to show up a few days after the incident. This warrants a visit to a trained health care provider for guidance on activity restrictions, rehabilitation strategies for optimal healing, and a safe plan for RTP.
My next week’s blog will discuss successful rehabilitation strategies to minimize long term adverse effects, provide education and use a systematic approach to evaluating safety in returning to activities.
Have you been told your balance issues are “just your age?”
Yes, balance does decline with age, in general. It is also true that there is quite a bit one can do (and easily incorporate into every day activities) to slow this down and actually improve balance. For most people, this translates to a better quality of life, more confidence to remain active, and reduced risk for falls. The important piece of information you must know is that a proper assessment of your balance issues allows you to have a targeted home program that is meant just for you. It is not “one size fits all.” Some people can practice standing on one leg all day long but their true issue may not be addressed. Just a short list of things that disrupt balance are back and orthopedic injuries, prior ear infections, viruses, medications, peripheral neuropathy, and vestibular issues. When a thorough exam is completed by a skilled health care provider, often there is successful, efficient intervention that helps dramatically.
